The Patient This ECG was obtained from a 28-year-old woman who was found in her home, unresponsive. She was hypotensive at 99/35. No one was available to provide information about past medical history or the onset of this event.
Before you read my comments, pause to look at the ECG and see what YOU think. We would welcome comments below from all our members!
The ECG This ECG is quite challenging, as it illustrates the helpfulness of ECG changes in patient diagnosis, and also points out how important clinical correlation is when the ECG suggests multiple different problems. Forgive me in advance, but there is a lot to say about this ECG.
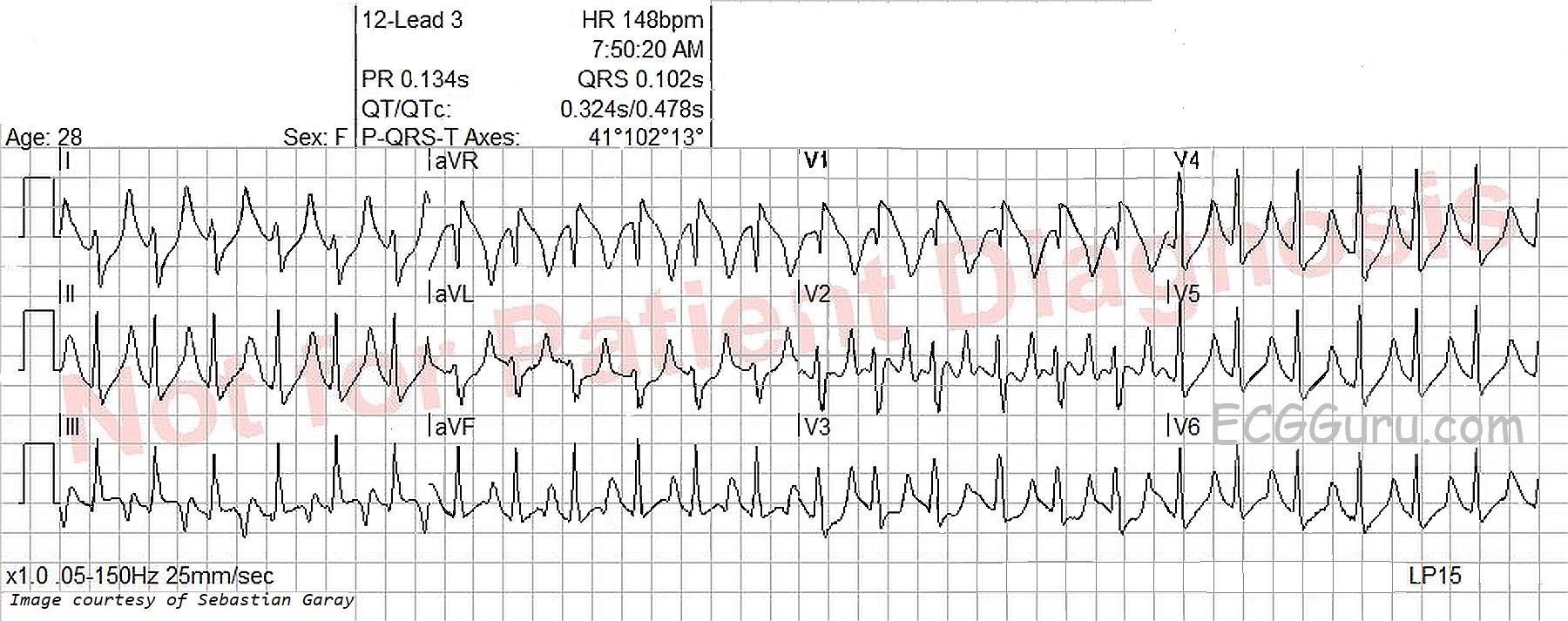
The heart rate is 148 bpm, and the rhythm is regular, although not perfectly. P waves are not seen, even though the ECG machine gives a P wave axis and PR interval measurement. The rate is fast enough to bury the P waves in the preceding T waves, especially if there is first-degree AV block. Differential dx: sinus tachycardia, PSVT, atrial flutter. The very slight irregularity points more towards sinus tachycardia. The rate of nearly 150 suggests atrial flutter with 2:1 conduction, but the only lead that looks remotely like it has flutter waves is V2. The lack of an onset or offset of the rhythm makes it difficult to diagnose PSVT with any certainty.
The ECG machine measures the QRS complex at .102 seconds (102 ms). I don’t believe this is correct, as the QRS has an additional wave due to right bundle branch block pattern, and the machine did not count this terminal wave. I measure the actual QRS duration at closer to .12 seconds (120 ms). The J point, or end point of the QRS complex, is difficult to see in most of the leads because of slurring from the QRS to the ST segment.
Differential dx: There are some signs of right ventricular failure on this ECG, but ECG is not 100% accurate for determining right heart strain. The ECG evidence must be confirmed by clinical correlation. In a young person with sudden onset of right heart failure signs, one must consider pulmonary embolus. Some, but not all, of the ECG signs that can be associated with pulmonary embolism are:
· Sinus tachycardia (44%)
· Right bundle branch block or incomplete RBBB (18%)
· Right ventricular strain: T wave inversion in right precordial leads and inferior leads (only present here in V1 and Lead III, which is often normal).
· Right axis deviation (16%). Present here, but not severe at around 100 degrees.
· S1 – Q3 – T3 the “classic” but not often present, sign of pulmonary embolism. The S wave in I may simply be the RBBB and the Q wave with T wave inversion may be a normal variant.
· Non-specific ST segment and T wave changes (50%)
· P pulmonale (we cannot see P waves)
There are also ST and T wave changes that resemble Brugada Syndrome, a genetic disorder of the sodium channel that can cause sudden death. Illness can unmask the ECG changes that point to Brugada syndrome, but also there are conditions that cause similar ECG changes without the patient actually having a channelopathy. The shape of the ST and inverted T wave in V1 here are “Brugada like”. In Brugada Syndrome, those changes are usually seen in V1 and V2.
The loss of P waves and the tall, peaked T waves with narrow bases are indicative of hyperkalemia. It is difficult to determine just from the ECG how far along the patient is in serum potassium levels, but widening of the QRS with loss of voltage is a dire sign. Because hyperkalemia can progress swiftly to a “sine wave” pattern, it is crucial to make the diagnosis and begin treatment as soon as possible. Usually, the serum K is high because the K has moved out of the intracellular space and entered the serum. Rather than remove K from the body, it is necessary to “push” it back into the cells, where it rightly belongs.
And, to make matters even more confusing, this ECG show signs of drug toxicity, specifically sodium channel blocker overdose. Tricyclic antidepressants and some antiarrhythmics fall into this broad category. Remember, this patient was found unresponsive, and we have no remote OR recent medical history. Everything is on the table. ECG signs of sodium channel blocker OD include:
· Sinus tachycardia
· Wide QRS complex
· Prolongation of the PR interval or QT interval
· Right bundle branch block
· Brugada pattern
Hospital Follow Up At this time, we have only a preliminary follow up report. Notably, this young woman was found to be in diabetic ketoacidosis, with a blood glucose level of 1,332 mg/dL! As a result, she was also hyperkalemic, with a serum potassium of 8.2. The severe dehydration and acidosis of DKA cause sinus tachycardia.
Thanks to Sebastian Garay for donating this interesting ECG.
