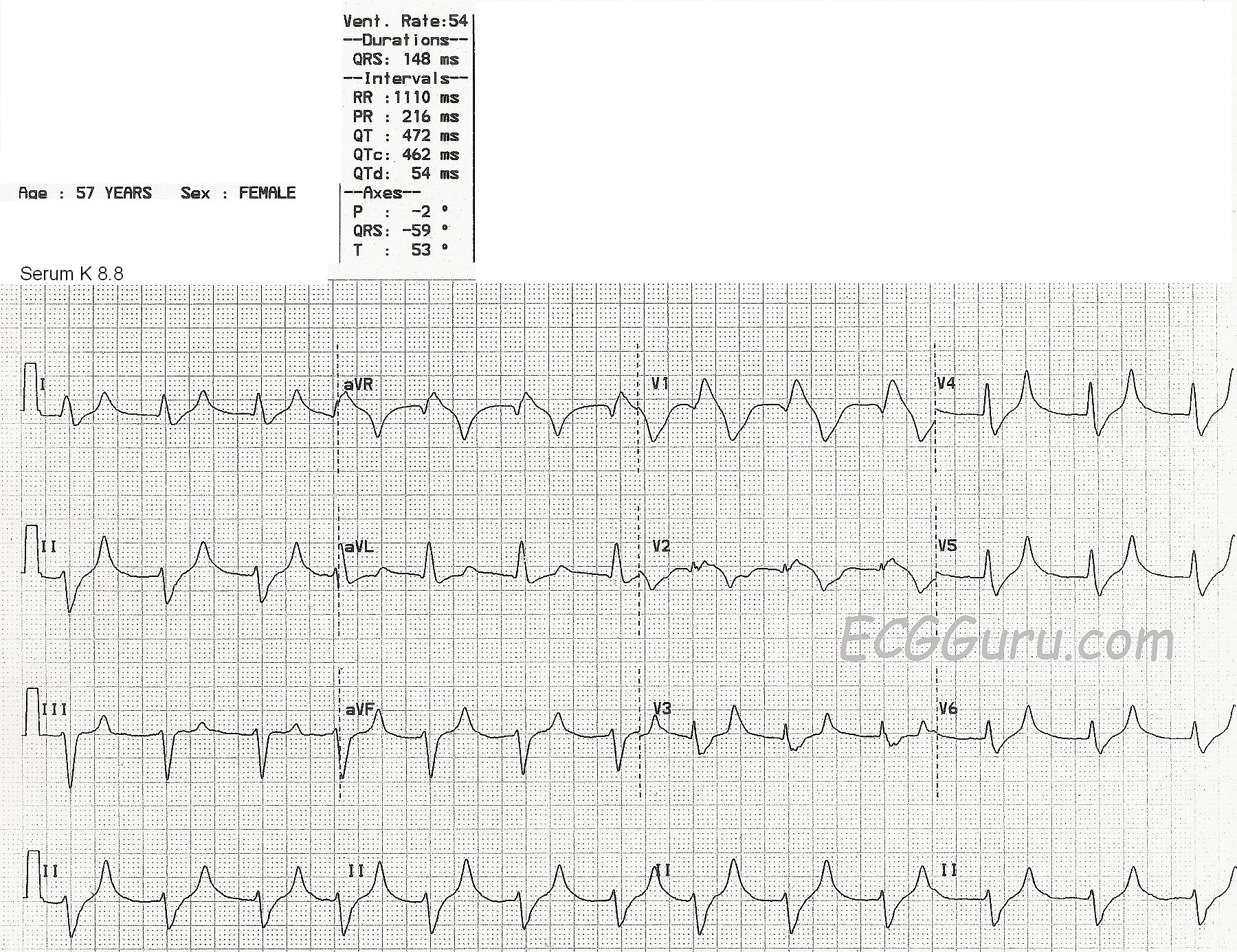
This ECG is from a 57-year-old woman with extreme weakness. We do not know her medical history or complete lab results, except that her serum potassium level was 8.8 mEq/liter at the time of this ECG.
This ECG shows a fairly regular rhythm at about 75 bpm, with a few early beats raising the rate slightly. (Even though the machine's interpretation lists the rate as 54 bpm. The QRS duration is listed at 148 ms (.148 seconds), but it appears wider. It is difficult to see the excact location of the J point because the QRS slurrs into the ST segment. Even though the ECG machine reports a P wave axis and a PR interval, P waves are not visible.
The QRS morphology appears to be an atypical right bundle branch block and left anterior hemiblock pattern. The T waves in leads I, II, aVF, and V3 through V6 are narrow, tall and peaked.
Potassium is primarily an intracellular electrolyte. It is necessary for proper electrical functioning of the heart. Extracellular serum potassium can rise due to renal failure, or taking potassium supplements, potassium-sparing diuretics, or ACE inhibitors. Occasionally, serum K levels may be artificially elevated by drawing the blood with too much syringe pressure, or using too small a needle, as the red blood cells can be damaged and release intracellular K into the serum.
ECG signs may vary among people with hyperkalemia, but in general:
Serum K levels of 5.5 mEq/L or greater can cause repolarization abnormalities like tall, peaked T waves.
Serum K levels of 6.5 mEq/L or greater cause progressive paralysis of the atria. The P waves will lose amplitude, widen and flatten. The PR segment will lengthen. Eventually, the P waves will disappear.
Serum K levels of 7.0 mEq/L or greater can cause conduction abnormalities. The QRS will widen and the rate will slow. There may be bundle branch blocks or fascicular blocks. The QRS morphology will be bizarre - not necessarily showing a typical bundle branch block pattern. AV blocks may occur, with either ventricular or junctional escape rhythms.
As the patient's condition worsens and the serum potassium rises, the QRS and T waves lose amplitude, widen, and may seem to blend together.
At levels above 8.0 mEq/L, we may see what looks like a bizarre idioventricular rhythm, or a sine wave pattern. This sine wave pattern signals cardiac arrest is imminent.
For a comprehensive discussion of hyperkalemia on the ECG with many examples of the different phases, go to Life In The Fast Lane. Ed Burns has compiled a very instructive collection of ECGs that illustrate the progression of this deadly condition.
Dr. Steve Smith's blog has several very good discussions on the subject. For a comparison of tall T waves caused by several factors, including hyperkalemia, go to Dr. Smith's Blog.
